Overview
Under Section 2799B-6 of the Public Health Service Act, effective January 1, 2022, health care providers and health care facilities are required to inform individuals who are not enrolled in a plan or coverage or a Federal health care program, or not seeking to file a claim with their plan or coverage both orally and in writing of their ability, upon request or at the time of scheduling health care items and services, to receive a “Good Faith Estimate” of expected charges.
The Departments of the Treasury, Labor, and Health and Human Services (collectively, the Departments) have issued interim final rules titled the “Requirements Related to Surprise Billing. In the interim final rule, HHS requires health care providers and health care facilities to provide a good faith estimate of the total expected charges to individuals who are not enrolled in a plan or coverage or a Federal health care program (uninsured individuals), or individuals who are enrolled but not seeking to file a claim with their plan or coverage (self-pay individuals) of the expected charges they may be billed for receiving certain health care items and services upon scheduling items and services, or upon the request of such individual. The authority for this requirement is PHS Act section 2799B-6 and the interim final rule at 45 CFR 149.610. Section 45 CFR 149.610(c), establishes requirements for the content that must be included in a good faith estimate that is issued to an uninsured (or self-pay) individual. Per 45 CFR 149.610(c)(1), all of the required elements must be included in the good faith estimate that the convening provider or convening facility issues to the uninsured (or self-pay) individual. As specified in 45 CFR 149.610(b)(1) and (2), the good faith estimate information submitted by co-providers or co-facilities must also be included as part of the good faith estimate issued to the uninsured (or self-pay) individual.
Creating a Good Faith Estimate Document or Template
The table below identifies data elements that health care providers and facilities, must include in the good faith estimate beginning on January 1, 2022. From January 1, 2022 through December 31, 2022, HHS will exercise its enforcement discretion in situations where the good faith estimate does not include expected charges for items and services from a co-provider or co-facility. data elements must be provided by a co-provider or co-facility beginning January 1, 2023.
|
Data Elements by Convening Provider or Facility
|
Description
|
|---|---|
|
Patient name and date of birth
|
First name, last name, and date of birth for the uninsured (or self-pay) individual receiving items or services.
|
|
Description of the primary item or service in clear and understandable language (and if applicable, the date the primary item or service is scheduled)
|
A description of the item or service to be furnished by the convening provider or facility (as defined for purposes of 45 CFR 149.610) that is the initial reason for the visit.
|
|
Items and services reasonably expected to be furnished for the period of care
|
An itemized list of the items and services, grouped by each provider or facility, reasonably expected to be furnished to the uninsured (or self-pay) individual, reasonably expected to be provided for the primary item or service, and items and services expected to be furnished in conjunction with and in support of the primary item or service, for that period of care including: (1) those items and services expected to be furnished by the convening provider or facility, and (2)those items and services expected to be furnished by co-providers or co-facilities, for the period of care.
|
|
Service codes
|
Description of an item or service using the Current Procedural Terminology (CPT), Healthcare Common Procedure Coding System (HCPCS), Diagnosis-Related Group (DRG), or National Drug Code (NDC) codes.
|
|
Diagnosis codes
|
The code that describes an individual’s disease, disorder, injury, and other related health conditions using the International Classification of Diseases (ICD) code set.
|
|
Expected charges
|
Expected charges associated with each listed item or service.
|
|
Names of providers and facilities
|
First name, last name, and title of providers. Facilities legal name as written on their business license.
|
|
Tax ID Number
|
Provider or facility’s taxpayer identification number (TIN), employer identification number (EIN), or federal tax identification number (FTIN) issued by the Internal Revenue Service.
|
|
National Provider Identifier
|
Provider or facility National Provider Identifier
|
|
List of items and services requiring separate scheduling
|
A list of items and services that the convening provider or convening facility anticipates will require separate scheduling and are expected to occur either prior to or following the expected period of care for the primary item or service. The good faith estimate must include a disclaimer directly above this list that states that separate good faith estimates will be issued to an uninsured (or self-pay) individual upon scheduling of the listed items and services; for items and services included in this list, information such as diagnosis codes, service codes, expected charges and provider or facility identifiers need not be included as that information will be provided in separate good faith estimates upon scheduling of such items and services.
|
|
State(s) and office or facility location(s)
|
Physical address, including street name and number, city, state, and zip code for all providers and facilities involved in the expected period of care.
|
|
Disclaimer stating that good faith estimate is an estimate and subject to change
|
Disclaim informing the uninsured (or self-pay) individual that the information provided in the good faith estimate are estimates and not the final overall total charges.
|
|
Disclaimer stating that there may be additional items or services not contained in the good faith estimate
|
Disclaimer informing the uninsured (or self-pay) individual that additional items and/or services that are not in the good faith estimate may be recommended by the convening provider as part of the course of care, that must be scheduled separately and are not reflected in the good faith estimate (such as rehabilitation therapies or other post treatment items or services) and information regarding how an uninsured (or self-pay) individual can obtain a good faith estimate for such items or services.
|
|
Disclaimer of their right to initiate the patient-provider dispute resolution process
|
Disclaimer providing the uninsured (or self-pay) individual of their right to initiate the patient-provider dispute resolution process if the actual billed charges are $400 more than the expected charges included in the good faith estimate.
|
|
Disclaimer that the good faith estimate is not a contract.
|
Disclaimer stating that the good faith estimate is not a contract or does not require the uninsured (or self-pay) individual to obtain the items and services from any of the providers or facilities identified on the good faith estimate.
|
|
Data Elements for Co-Providers or Co-Facilities to Convening Providers or Convening Facilities (this may not apply to your facility)
|
Description
|
|
Patient's Name and Date of Birth
|
First name, last name, and date of birth for the uninsured (or self-pay) individual receiving items or services
|
|
Items and services expected to be furnished by co-provider or co-facility
|
Items or services that are reasonably expected to be furnished in support of and in conjunction with the primary item or service for the period of care.
|
|
Service Codes
|
Description of an item or service using the CPT code, HCPCS, DRG, or NDC codes.
|
|
Diagnosis Codes
|
The code that describes an individual’s disease, disorder, injury, and other related health conditions using the ICD code set.
|
|
Expected Charges
|
Expected charges associated with each listed item or service.
|
|
Names of co-providers and co-facilities
|
First name, last name, and title of co-providers. Co-facilities legal name as written on their business license.
|
|
Tax ID Number
|
Provider or facility’s TIN, EIN, or FTIN issued by the Internal Revenue Service.
|
|
National Provider Identifier
|
Provider or facility's National Provider Identifier
|
|
State(s) and office or facility location(s)
|
Physical address, including street name and number, city, state, and zip code.
|
|
Disclaimer that the good faith estimate is not a contract
|
Disclaimer stating that the good faith estimate is not a contract and does not require the uninsured (or self-pay) individual to obtain the items and services from any of the providers or facilities identified on the good faith estimate.
|
Creating & Sending a Good Faith Estimate using the Client Portal
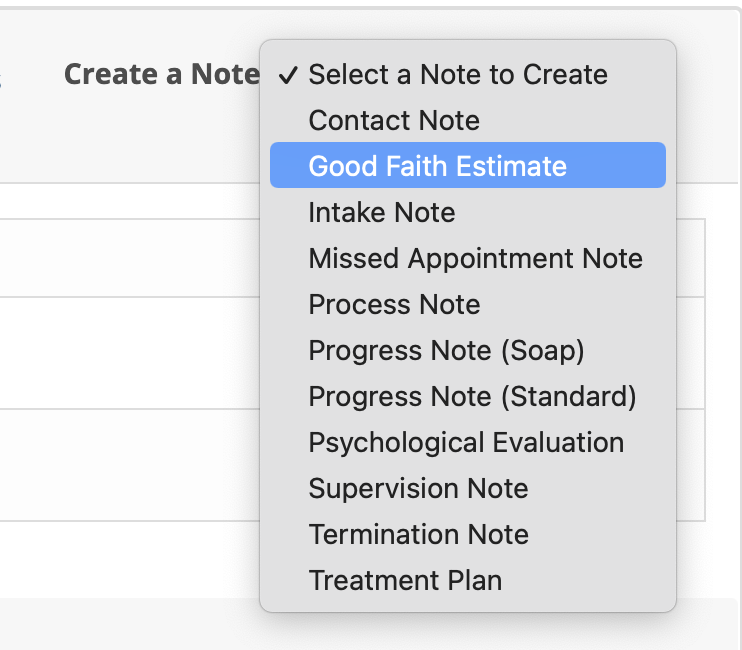
You can create and send a Good Faith Estimate within TherapyMate to a client using the Client Portal. Go to the client's Notes & Document tab and click on the Create a Note drop down shown below. You will see an option for Good Faith Estimate in the list.
Select the Good Faith Estimate option and a template will appear. Most of the data fields will automatically be filled in for you if the clients information page contains the data already.
You will need to complete the following:
1. Enter the Description of services
2. Add the service codes you will provide by clicking the + Add Service link. Add as many service codes as you like.
3. Estimate the total cost of all services that will be provided. If unknown, maybe you could give a typical example of what the client could expected. The box can contain alpha and numeric characters. In the disclaimer area you'll notice a sentence that says: Total charges will depend on how many appointments are scheduled and completed over time.
4. Choose whether or not the client has an appointment. If the client does have an appointment already scheduled, choose the date of the appointment from the First session scheduled at drop down.
5. Add the service location where the services will be delivered by the clinician
6. The disclaimer is provided using the recommended language. You can add additional information to this area as needed. The information you add will be relevant for this one client only. The changes are not saved for other clients.
7. Choose the diagnosis codes if it is known at this time. If you don't add any diagnosis codes, there is a sentence on the completed document that says: Please note: It may not be possible to provide the Diagnosis(s) until the clinician has met with the client.
Click the blue Add button when done. A preview of the Good Faith Estimate will appear next. Click the Send to Client button to send the estimate to the client via the Client Portal.
Please Note: The client must have been invited to the portal prior to you sending the estimate. The client must have a client portal username and password to login.
The client will receive an email that asks them to login into the portal to view and sign the Good Faith Estimate. When the estimate is signed and saved, a copy will be automatically added to the client's documents area at the bottom of their Notes & Documents page.
Office Signage
Information regarding the availability of a “Good Faith Estimate” must be prominently displayed on the convening provider’s and convening facility’s website and in the office and on-site where scheduling or questions about the cost of health care occur. Here is some text that you might consider for the sign you are required to post in the office:
Good Faith Estimate-No Surprises Act
You have the right to receive a “Good Faith Estimate” explaining how much your medical care will cost
Under the law, health care providers need to give patients who don’t have insurance or who are not using insurance an estimate for medical items and services. If this applies to you:
•You have the right to receive a Good Faith Estimate for the total expected cost of any non-emergency items or services. This includes related costs for medical tests, prescription drugs, equipment, and hospital fees.
•Make sure your health care provider gives you a Good Faith Estimate in writing at least 1 business day before your medical service or item. You can also ask your health care provider, and any other provider you choose, for a Good Faith Estimate before you schedule an item or service.
•If you receive a bill that is at least $400 more than your Good Faith Estimate, you can dispute the bill.
•Make sure to save a copy or picture of your Good Faith Estimate.
For questions or more information about your right to a Good Faith Estimate, visit www.cms.gov/nosurprises or call [practice phone number].
Update Your Website
Add the following text to your website in an appropriate location:
Under Section 2799B-6 of the Public Health Service Act, health care providers and health care facilities are required to inform individuals who are not enrolled in an insurance plan or coverage or a Federal health care program, or not seeking to file a claim with their plan or coverage, a Good Faith Estimate of expected charges, both orally and in writing or upon request or at the time of scheduling health care services.
What are the consequences of not providing the notice and/or the GFE when required to do so?
The NSA enforcement was published September 16, 2021. It specifies the investigatory process and the imposition of civil money penalties of up to $10,000 per violation. Comments on the proposed rule were due October 18. The final enforcement rule should be published within the next few months.
Additional Resources
PYA-No Surprises Implementation Guide
Centers for Medicare & Medicaid Services
CMS has published a standard form for providers to use in providing GFEs and an explanation of the specific data elements to be included in the estimate, available here (included in the ZIP file as Appendices 2 and 11). Again, use of the standard form is not mandated, but CMS will consider its use good faith compliance with the requirement to inform an individual of expected charges.